Did you know that between 2008-2015, only 2% of all Autism-focused health research was about adults over the age of 18?
This is a critical gap in our pursuit of health equity.
Our team—led by an Autistic Founding Director and partnered with a number of Autist-scholars and Autist-educators—is increasingly concerned with the lack of Autistic-led gender and sexual health research. Indeed, being excluded and ignored has dire consequences for Autistic health and wellbeing!
Gender and sexual health, specifically, are key mechanisms through which Autists experience erasure, discrimination, and violence. Emerging research suggests that transgender and gender expansive (TGE) people are 3-6x more likely to be Autistic than cisgender people, and Autistic people are 3-5x more likely to be LGBQA+ (lesbian, gay, bisexual, queer, asexual, sexually-expansive) than the “general population”. Despite this, Autism is nearly always excluded from sexual health education curricula and training, including comprehensive K-12 models.
At the same time, despite Autists being more likely to experience intimate partner and sexual violence, only seven states provide sexual health services within their home-based disability health programs. Parents of Autistic youth often report that they believe their children should not be given any information about gender, sexuality, or relationships; and/or report lacking the necessary education and training to handle these conversations.
So, what are we going to do about it?
-
To address both the gap in the science of engaging Autists and the critical health equity concern of GSH, this study will integrate Autistic lived experience leadership into the ADAPT-ITT model.
The Assessment, Decision, Adaptation, Production, Topical experts-integration, Training, and Testing (ADAPT-ITT) model is said to “directly involve members of [a] new target population, key stakeholders, and agency staff from the initial phase to the last phase” of an eight-phase process guiding the creation of culturally-responsible, methodologically rigorous, scientifically sound health prevention and early intervention (PEI) programming.
It has been used extensively in HIV/STI PEI efforts, preliminarily for dating violence and sexual assault PEI programming, and, in a few emergent studies, with Autistic youth and/or LGBTQ+ populations. As such, it holds promise for use in this study.
Critically, integrating lived experience leadership into the ADAPT-ITT model is novel: a recent systematic review found that only 18% of studies using ADAPT-ITT for trauma-related PEI included community shared decision-making across all phases, and it is unclear if any supported the full project/programmatic control of people with lived experience.
-
To co-develop a GSH PEI (the pilot project). The Research Team (PI, Research Manager, Engagement Coordinator, Graduate Student Research Assistant, and Study Team Expert Consultants) will convene a group of 12 PPs in a Community Engagement Studio.
Across the first 30 months of the project, we will work together to co-develop the gender and sexual health PEI program. Given the social determinants impacting Autists’ health, we will prioritize the recruitment and participation of community members who are BIPOC, 2SLGBTQIA+, elders, c/s/x (consumers/survivors/ex-patients), intellectually disabled, and/or non-speaking.
During the ADAPT-ITT process, these 12 Autists will determine the size, scope, and primary data collection necessary to effectively adapt a GSH PEI program; as such, specific details on the pilot project’s study population/sample are not yet known. The image below outlines the key methods typically employed for ADAPT-ITT projects. Additional documentation on appropriateness and efficacy of Community Engagement Studios and ADAPT-ITT methodologies can be provided upon request.
-
We will work with together to pilot the program and then produce a report, toolkit, or similar guidance for translation and dissemination on the framework and logistical steps for conducting lived experience-led ADAPT-ITT projects.
The last stage of the ADAPT-ITT process is to pilot gender and sexual health PEI program for Autists, measure its impacts, and produce a dissemination report for vested and new partners (Autists, families/caregivers, health care providers, GSH researchers, community advocates, etc.).
During the pilot phase, in addition to measuring the PEI’s impact on gender and sexual health in the short-term, we will also be assessing the robustness, usability, acceptability, and efficacy of engagement methods and approaches (e.g. the impact of the lived experience leadership ADAPT-ITT hybrid methodology).
While not the focus of this particular project, we imagine our resulting PEI could be referenced educationally and/or implemented in certain settings as-is by those community members and partners; and, if successful, we plan to test the PEI program in a future pragmatic randomized control effectiveness trial.
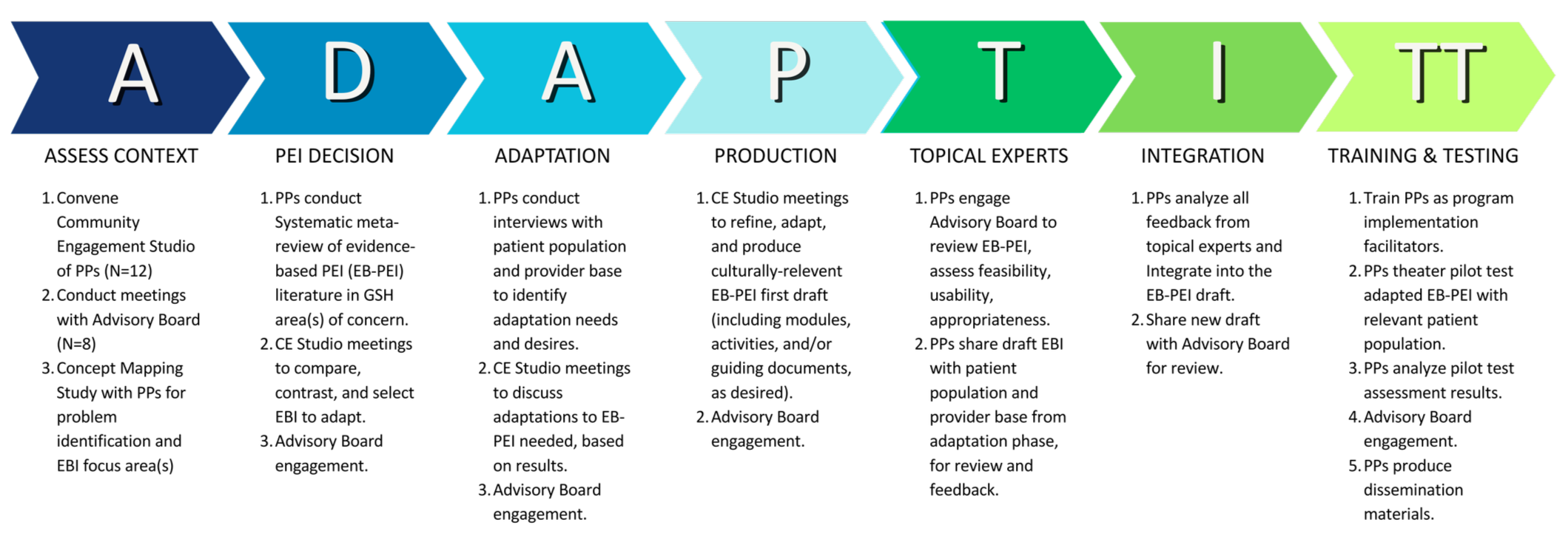
“PP” stands for “Patient Partner” - this graphic comes specifically from an under review PCORI project, which requires the use of this terminology. Note that we understand patient partners as community members and expert consultants in our work, regardless of this language choice!